Sarcopenia is no longer viewed as a normal, unavoidable part of aging. It is a progressive muscle disease associated with reduced strength, impaired mobility, falls, disability, loss of independence, and higher health risk. The revised European consensus definition places low muscle strength at the center of diagnosis, with low muscle quantity or quality confirming the diagnosis and poor physical performance indicating severe sarcopenia [1].
For healthcare providers, the practical challenge is familiar. The patients who need muscle stimulation most are often the least able to tolerate aggressive exercise. They may have joint pain, poor balance, fear of falling, cardiometabolic disease, neuropathy, frailty, or recent deconditioning. Low-intensity vibration may help fill this gap. It is not a replacement for resistance training, but it may provide a low-load neuromuscular stimulus for patients who cannot yet perform enough conventional exercise to drive adaptation.
Why Sarcopenia Is More Than Muscle Loss
Sarcopenia involves more than reduced muscle size. It also includes impaired neuromuscular activation, reduced motor unit recruitment, slower reaction time, diminished balance, and poorer coordination. These changes explain why a patient may have difficulty rising from a chair, initiating gait, recovering from a trip, or maintaining confidence while walking.
Exercise remains the cornerstone of sarcopenia management, particularly resistance training. However, systematic reviews show that exercise interventions often improve strength and physical performance more reliably than muscle mass itself [2]. That distinction is clinically important. In older adults, better function may matter more than measurable hypertrophy.
Low-intensity vibration fits this functional model. Rather than trying to build muscle mass directly, it may support muscle performance by stimulating sensory-motor pathways and improving readiness for movement.
How Low-Intensity Vibration May Support Muscle Function
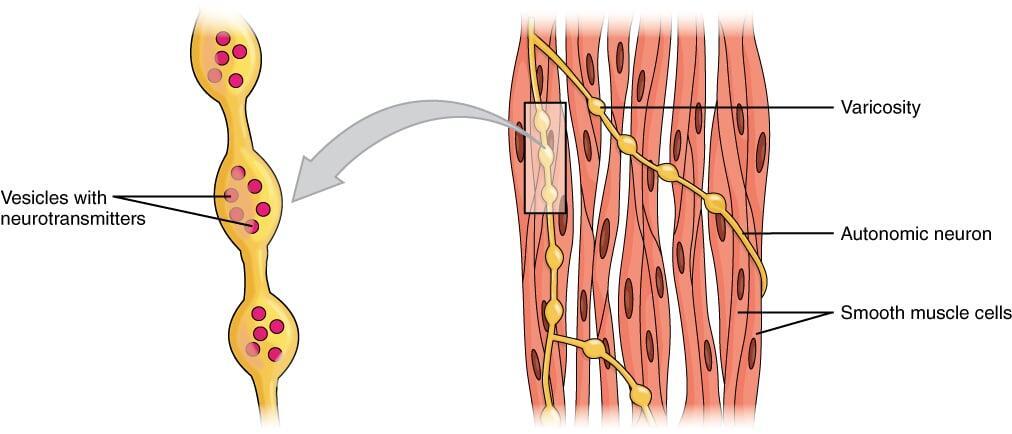
Vibration platforms deliver rapid mechanical oscillations through the feet or body. These signals can stimulate muscle spindles, proprioceptive pathways, and reflexive neuromuscular activity. In a sarcopenic patient, this may provide a low-threshold stimulus to the lower extremities without requiring heavy loading.
A systematic review and meta-analysis of vibration therapy in older adults with sarcopenia concluded that vibration therapy may improve muscle strength and physical performance, although effects on muscle mass are less consistent [3]. This aligns with the clinical reality of sarcopenia care: improving chair rise ability, gait speed, and balance may be more immediately relevant than increasing lean mass.
A 2025 study comparing 12-week whole-body vibration training with resistance training found that both improved physical condition in older adults with sarcopenia, while resistance training had stronger effects on muscle strength. The authors concluded that vibration may be an alternative option for patients who have difficulty performing conventional resistance training [4].
Low-Intensity Vibration as a Bridge to Exercise
The strongest clinical role for low-intensity vibration is as a bridge intervention. Many sarcopenic patients are not ready for progressive resistance exercise at the start of care. They may need a preparatory phase that improves confidence, sensory input, standing tolerance, and lower-extremity activation.
Practical applications include:
- Seated use with feet on the platform for very deconditioned patients
- Supported standing for balance-challenged patients
- Short sessions before therapeutic exercise to improve neuromuscular readiness
- Adjunctive use before gait training or sit-to-stand practice
- Maintenance support for patients who are inconsistent with home exercise
- Providers should frame vibration as part of a broader plan that includes protein optimization, vitamin D sufficiency when indicated, resistance training, balance work, medication review, and fall-risk management.
Patient Selection
Low-intensity vibration may be most appropriate for:
- Older adults with probable or confirmed sarcopenia
- Patients with low gait speed or poor chair-rise performance
- Frail patients who cannot tolerate higher-force exercise
- Sedentary patients beginning a movement program
- Patients with fear of falling or low balance confidence
- Individuals transitioning from inactivity to active rehabilitation
- It may be less appropriate for patients who can already tolerate progressive resistance training and need higher overload to improve strength. In those cases, vibration may still be useful as an adjunct, but it should not displace evidence-based strengthening.
Safety and Documentation
Low-intensity vibration is generally well tolerated when used appropriately, but screening is still required. Contraindications may include acute fracture, active deep vein thrombosis, unstable cardiovascular disease, severe vestibular instability, pregnancy, and certain implanted electronic devices. Patients with advanced osteoporosis, recent surgery, or complex neurologic disease should be supervised closely.
Documentation should be functional. Track baseline and follow-up measures such as gait speed, Timed Up and Go, 30-second chair stand, grip strength, balance confidence, fall history, session tolerance, and adherence. These outcomes align with sarcopenia definitions and clinical goals [1].
Takeaway for Healthcare Providers
Low-intensity vibration should not be marketed as a stand-alone sarcopenia cure. The evidence is more nuanced. It appears most defensible as a low-load adjunct that may improve strength-related performance, balance readiness, and functional mobility in older adults who cannot tolerate sufficient conventional exercise.
For sarcopenic patients, the clinical objective is often not maximal muscle growth. It is restoring enough function to stand, walk, train, and live with less risk. Low-intensity vibration may be a useful step in that progression.
To learn more about whole body vibrationemail usor call Rob at 860-707-4220.
References
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16-31.
- Bao W, Sun Y, Zhang T, et al. Exercise programs for muscle mass, muscle strength and physical performance in older adults with sarcopenia: a systematic review and meta-analysis. Aging Dis. 2020;11(4):863-873.
- Wu S, Ning HT, Xiao SM, et al. Effects of vibration therapy on muscle mass, muscle strength and physical function in older adults with sarcopenia: a systematic review and meta-analysis. Eur Rev Aging Phys Act. 2020;17:14.
- Zhuang M, Liu Y, Li J, et al. Effects of 12-week whole-body vibration training versus resistance training in older people with sarcopenia: a randomized controlled trial. Front Physiol. 2025.